By Owokole, Adebusola
Early in the twentieth century, peptic ulcers were thought to be caused by emotional stress and spicy foods. As a result, people were treated with bed rest and a bland diet, but they often fail to get better. Later in the Century, the disease was blamed on excess stomach acid. People were treated with medicines that counteract acid or block its production, which made them feel better for a little while. The ulcers and the pain they caused however, often came back.
It is the most common ulcer of the gastrointestinal tract. It is usually acidic and thus extremely painful. Many peptic ulcers arise in the duodenum, the first part of the small intestine, just beyond the stomach. Most are generally benign. Small ulcers may not be noticeable, whereas large ulcers are medical emergencies. It happens to any age and both sexes. There are 500,000 to 850,000 new cases of the diagnosed each year.
DEFINITION
Peptic ulcer disease refers to painful sores or ulcers in the lining of the stomach or first part of the small intestine, called the duodenum.
CLASSIFICATION
Duodenum: Duodenal ulcer
Esophagus: Esophageal ulcer
Stomach: Gastric ulcer
Meckel’s diverticulum
CAUSES
BACTERIAL INFECTIONS: Helicobacter Pylori is one of the most common causes of peptic ulcer.It colonises the stomach and the body’s immune system is unable to clear the infection. Normally, the stomach makes acid as part of the digestive process. The sensitive lining of the stomach and duodenum is protected from this acid by a mucous coating. H. Pylori bacteria cause ulcers by weakening this mucous coating, which allows the acid to get through creating holes in the lining beneath.
DRUGS: Can also be caused or worsened by long-term use of certain drugs:
NSAIDS: Painkillers, such as Aspirin, Naproxen, Ibuprofen.
Glucocorticoids: Dexamethasone, Prednisolone. NSAIDs interfere with the stomach’s ability to protect itself against the acid. A weakening of the stomach lining caused by continuous use of an anti-inflammatory.
TUMOURS
About 4% of gastric ulcers are caused by a malignant tumour, so multiple biopsies are needed to exclude cancer. Tumors of the acid producing cells of the stomach that increases acid output {Zollinger –Ellison Syndrome}.
Usually, children and elderly do not develop symptoms unless symptoms have risen.
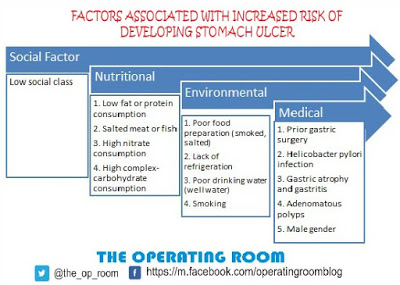
Suggested risk factors: Diet: Spice consumption, caffeine, coffee, carbonated drinks.
Excessive stress
Smoking
DIAGNOSTIC EVALUATION
BARIUM X-RAY: The person drinks a chalky liquid that makes the stomach, duodenum, and any ulcersd show up clearly on an X-ray image.
GASTROSCOPY: The person is given medicine to relax. Then, a thin lighted tube is passed through the person’s stomach and down the throat to the stomach and duodenum. This tube has a tiny camera on the end that allows visualization of the inside of stomach. Usually, ordered if symptoms do not resolve after a few weeks of treatment. It is used to directly visualize the location and severity. Biopsies are usually taken. Another test may be conducted 6-12 months after taking treatment to confirm eradication of bacteria.
SIGNS AND SYMPTOMS
Abdominal pain: Epigastric, strongly correlated to mealtimes. In case of duodenal ulcers, the pain appears about threehours after a meal. Pain may be misinterpreted as hunger, indigestion or heartburn. The pain may flare at night and can temporarily be relieved by eating or by taking anti-acid medication. Rarely, can lead to a gastric perforation, which leads to peritonitis, extreme, stabbing pain, and requires immediate surgery.
Burning or gnawing feeling in the stomach lasting between 30 minutes and 3 hours:
Bloating and abdominal fullness
Heartburn
Waterbrash: Rush of saliva after an episode of regurgitation to dilute the acid in oesophagus.
Nausea and copious vomiting
Loss of appetite and weight loss
Haematemesis: Vomiting of blood, that look like ‘coffee-grounds’, can occur due to bleeding directly from a gastric ulcer, or from damage to the oesophagus from severe/ continuing vomiting
Melena: Tarry, foul-smelling faeces due to presence of oxidized iron from haemoglobin
In duodenal ulcers, drinking milk, eating or taking antacids generally relieves the pain but , but it usually returns 2 to 3 hours later.
COMPLICATIONS
Gastro-intestinal bleeding: Occurs when the ulcer erodes one of the blood vessels in the stomach.
Perforation: A hole in the wall of the stomach created by erosion leads to spillage of stomach or intestinal content into the abdominal cavity. Pain is sudden, intense, rapid, may spread to the shoulders and intensify with deep breathing.
Penetration: When the ulcer continues into adjacent organs such as liver and pancreas
Gastric Outlet Obstruction: Narrowing of the pyloric canal caused by scarring and swelling. This leads to severe vomiting. Pain is piercing and persistent, may radiate to the back
Complications are accompanied by symptoms of low pressure, dizziness and fainting.
TRANSMISSION OF H. PYLORI INFECTIONS
Contaminated food
Contaminated ground water
Human Saliva { Kissing or Sharing food utensils}
TREATMENT
Combination of two or three antibiotics
• Amoxicillin + Clarithromycin + Metronidazole
• PPI: Omeprazole
• H2 Antagonists: Ranitidine and Famotidine
• Antacids
Eradication of H. Pylori usually leads to clearing of infection, relief of symptoms and eventual healing of ulcers.
Drugs are usually taken for one to two weeks
Surgical Intervention: Repair of perforation,, Selective Vagotomy.
HIGHLY ACIDIC FOODS: These vary among individuals
• Artificial sweeteners
• Chocolate
• White Bread
• Pork, Poultry
• Sugar, Jams
• Wheat flour
• Meat: Beef, Chicken
• Carbonated drinks
• Yoghurt
• Orange juice, lemon, lemonade, grape fruit, pineapple
• Tomato
• Raw Onion
• Yeast
• Pasta
• Wine, Liquor, tea, coffee
CONCLUSION
• Eat regularly. Don’t skip meals. Give your body fuel throughout the day. Eat smaller portions. Bigger is not always better, chew slowly.
• Get enough sleep. Get to bed earlier. Make sure your children get enough sleep.
• 0-2mths: 10-18hrs, 2mths-3yrs: 12-14 hrs, 3-5yrs: 11-13 hrs, 5-12yrs: 9-11hrs, Adolescents: 8.5-9.5 hrs, Adults: 7-9hrs.
Sources:
Atlas of Pathology
Eating, diet, and nutrition for peptic ulcer disease
Facts for peptic ulcer disease
Physiology of Medicine
The Merck Manuals