Definition
True vs. False aneurysms
A true aneurysm involves all three layers of the blood vessel wall. Whereas a false aneurysm consists of clot which has leaked from the true lumen and is surrounded by connective tissue. Femoral artery puncture, e.g. for angiography, is a common cause of false aneurysms.
Pathology of aneurysms
Degenerative: The idea of atherosclerosis causing AAA has been revised to a model that suggests degeneration due to an inflammatory process, leading to dilatation and subsequent plaque deposition. (Goldstone 1998)
MMP mediated. Especially 2 and 9
Infection: Classically syphilis. Septic embolisation (mycotic). Most studies report Staph. Aureus and Salmonella as the infective organisms.
Collagen diseases: Marfan’s syndrome / Ehlers-Danlos syndrome (esp. Type IV)
Congenital: Berry aneurysms present on the circle Willis.
Traumatic: blunt and sharp trauma
Iatrogenic e.g. after femoral artery puncture for angiograms
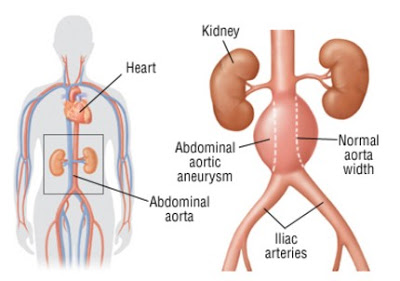
Abdominal Aortic Aneurysms
Prevalence is 7-8% in men aged over 65
Infra-renal aorta is commonest site of aortic aneurysm.
Remember most are asymptomatic. Over 50% will die of other causes with their AAA intact.
Affects 7% males and 2% females aged >65 and incidence is on the rise in the West.
Strong FHx. 20% males with AAA will have a first degree relative with a AAA.
Supra-renal extension occurs in 2-5%
Often found incidentally. Esp. USS for prostatism.
High association with aneurysms in other areas. Especially iliac and popliteal.
Main complication is rupture (cf. dissection which results from a intimal tear resulting in blood tracking down the vessel wall splitting the media.)
The annual rupture rate in the UK Small Aneurysm Trial (N = 2257, with about half in randomized arm and half in the registry) was 2.2% per year for the first 3 years of follow-up (Powell, 2001). The initial aneurysm diameter was 3-6 cm, and the mean was approximately 4.4 cm.
Remember that 25% of patients with AAA with have a popliteal / femoral aneursym
Examination
B-Mode USS
CT
MRA – Often not useful for AAA as only shows the lumen where there is blood flow.
AXR – remember to look for a rim of calcification
Treatment
Avoid emergency by treating electively.
Remember most patients are asymptomatic and operation carries reasonably high morbidity / mortality (2 – 5%).
Trials have shown two quantative measures.
Size ³ 5.5cm (UK) – 5cm USA
Increase in size ³ 0.5cm in 12 months
The UK Small Aneurysm Trial (1998) randomised just over 1000 patients with small (4 – 5.5 cm) aneurysms. There was no overall improvement in mortality in patients offered early surgery.
Cronenwett (J Vasc Surg 1990) suggested that COPD and HT increased risk of rupture and should be taken into account.
Overall 30 day mortality is ~ 5% (50% from IHD)
Emergency Treatment
Presentation can be with a variety of abdo pain radiating to back and groin. So always suspect in men aged >55 with renal colic.
Basic resuscitation – A B C
Insert at least two large-bore cannulae and start an IVI
Insert a urinary catheter
Analgesia
Cross match 6 units of blood
Take straight to theatre. Does NOT need investigating with USS / CT first!!
If systolic >100mmHg consider lowering BP with GTN etc